Flame-Retardant Heat-Shrink Tubing in Hospital and Medical Facilities

When a fire breaks out in a hospital, every second counts. Patients who cannot evacuate on their own, oxygen-rich environments that accelerate combustion, and a dense web of electrical systems running through every corridor combine to create one of the most unforgiving fire scenarios a facility can face. Flame-retardant heat-shrink tubing plays a role in this picture that is small in physical size but disproportionate in consequence — a few millimeters of polymer around a wire splice can mean the difference between a self-extinguishing insulation fault and a propagating cable fire.
This article examines why flame-retardant heat-shrink tubing is essential in medical environments, which standards govern its use, how material selection affects safety outcomes, and what procurement teams and specifying engineers should look for when sourcing tubing for healthcare applications.
Why Flame Retardancy Is Non-Negotiable in Medical Settings
A hospital’s electrical infrastructure is unlike any other building’s. Imaging equipment, ventilators, infusion pumps, patient monitors, surgical robots, and life-support systems operate around the clock, often concentrated in confined equipment racks and cable trays. Every termination, splice, and connector in these systems represents a potential ignition point. When an electrical fault occurs — a short circuit, an arc, a component overheating — the insulation materials immediately adjacent to the fault are the first line of defense against fire propagation.
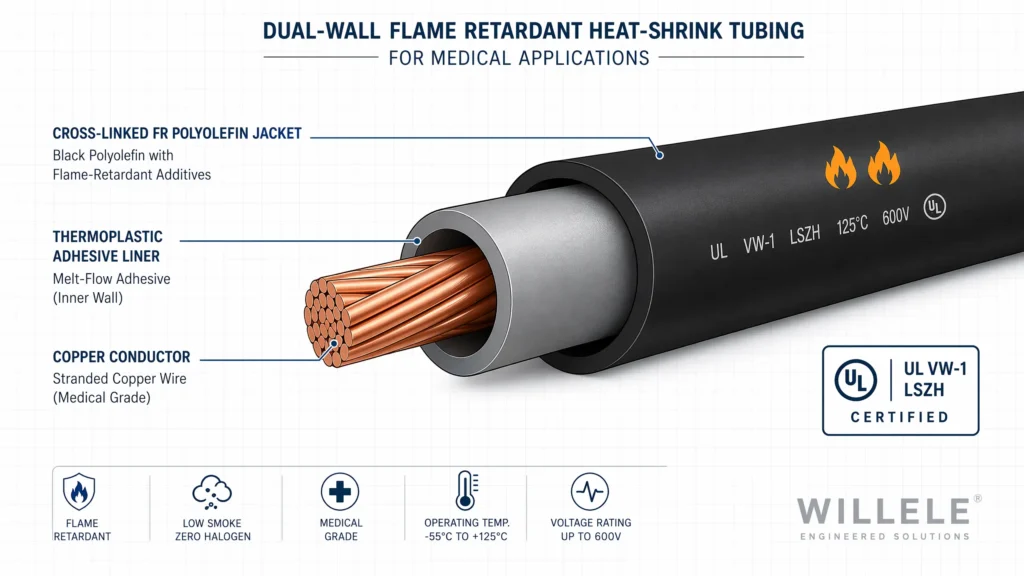
Standard polyolefin heat-shrink tubing without flame-retardant additives will ignite and continue burning once the external flame source is removed. Flame-retardant grades, by contrast, are formulated to self-extinguish within seconds. The widely recognized UL VW-1 vertical flame test requires the material to stop burning within 60 seconds and limits the extent of flame propagation along the specimen. In a hospital equipment rack where dozens of cables run in parallel, this self-extinguishing behavior can prevent a localized fault from becoming a room-scale emergency.
The regulatory landscape reinforces this requirement. NFPA 99, the Health Care Facilities Code, sets minimum standards for electrical systems in hospitals, nursing homes, and ambulatory care facilities. NFPA 70 (the National Electrical Code) imposes additional wiring and insulation requirements for patient care areas. Together, these codes create a framework in which every insulating material — including heat-shrink tubing — must contribute to the facility’s overall fire safety strategy rather than undermine it.
Standards and Certifications: What to Look For
Engineers specifying heat-shrink tubing for medical applications face a thicket of overlapping standards. The table below summarizes the most relevant ones and what each means in practice.
| Standard | What It Governs | Key Requirement | Relevance to Medical Facilities |
|---|---|---|---|
| UL 224 / VW-1 | Flame propagation on insulated wire | Self-extinguish within 60 seconds; no ignition of cotton indicator | Baseline flame retardancy for all heat-shrink tubing used in patient-care areas |
| UL 94 V-0 | Flammability of plastic materials | Self-extinguish within 10 seconds; no flaming drips | Required for enclosures and components inside medical devices per IEC 60601-1 |
| IEC 60601-1 Clause 11.3 | Fire enclosures of medical electrical equipment | Internal wiring must meet FV-1 or better flammability classification | Governs tubing used inside diagnostic and therapeutic equipment |
| IEC 60332-1 | Flame spread on single cables | Limits charred length and burning duration | Referenced by TE Connectivity for hospital-grade cable accessories |
| NFPA 99 | Electrical systems in healthcare facilities | Design, installation, testing, and maintenance of all electrical components | Covers the facility-level context in which the tubing operates |
| ISO 10993 | Biocompatibility of medical devices | Cytotoxicity, sensitization, and irritation testing | Required when tubing contacts patients or is used in medical device assembly |
| IEC 61249 | Halogen-free materials | Br < 900 ppm, Cl < 900 ppm, Br+Cl < 1500 ppm | Essential for enclosed and occupied spaces where toxic gas release is unacceptable |
A tube that carries a UL VW-1 mark but nothing else may be adequate for general-purpose use in a hospital’s back-office wiring. But for anything inside a medical device, inside a patient care area enclosure, or inside an operating room cable harness, the bar rises to include halogen-free composition, low smoke generation, and — where patient contact is possible — biocompatibility certification.
LSZH: Why Halogen-Free Matters More in Hospitals Than Anywhere Else
Conventional flame-retardant polymers rely on halogenated additives — brominated or chlorinated compounds — that interfere with the combustion chemistry. They work, but at a cost: when they burn, they release dense black smoke and corrosive hydrogen halide gases (HCl, HBr). In a hospital, this trade-off is unacceptable for three reasons.
First, smoke impairs visibility during evacuation. Hospital corridors during a fire emergency are already chaotic; thick, obscuring smoke from burning cable insulation can turn a navigable exit path into a lethal trap. Low Smoke Zero Halogen (LSZH) formulations reduce smoke density by an order of magnitude compared to halogenated alternatives.
Second, hydrogen halide gases are acutely toxic. They combine with moisture in the airways to form hydrochloric acid, causing severe respiratory injury. For patients already compromised — those in intensive care, on ventilators, or recovering from surgery — exposure to even low concentrations can be fatal.
Third, these same acid gases corrode electronic equipment far beyond the fire zone. A cable fire in one wing of a hospital can release HCl gas that travels through air-handling systems and damages sensitive electronics in adjacent departments, multiplying the financial and operational impact of the incident.
LSZH heat-shrink tubing addresses all three problems. It achieves flame retardancy through inorganic fillers — typically aluminium trihydrate (ATH) or magnesium hydroxide — that release water vapor when heated, an endothermic reaction that cools the material and dilutes combustible gases. The result is a tube that meets VW-1 or V-0 flame ratings while producing minimal smoke and no halogen acids. For hospitals, this has become the de facto specification for any heat-shrink tubing installed in occupied or enclosed spaces.
Material Types: A Performance Comparison
Not all flame-retardant heat-shrink tubing is created equal. The table below compares the four material families most commonly encountered in medical and healthcare applications.
| Property | Standard FR Polyolefin | LSZH Polyolefin | Dual-Wall FR (Adhesive-Lined) | Fluoropolymer (FEP/PVDF) |
|---|---|---|---|---|
| Flame Rating | VW-1 | VW-1 / V-0 | VW-1 | VW-1 / self-extinguishing |
| Halogen Content | May contain halogens | Halogen-free (< 900 ppm each) | Outer jacket may contain halogens | Halogen-containing (fluorine-based) |
| Smoke Density | Moderate | Very low | Moderate to high | Low |
| Temperature Range | -55°C to 135°C | -55°C to 125°C | -40°C to 125°C | -65°C to 200°C (FEP) |
| Shrink Ratio | 2:1, 3:1 | 2:1, 3:1 | 3:1, 4:1 | 1.3:1 to 2:1 |
| Dielectric Strength | ≥ 20 kV/mm | ≥ 20 kV/mm | ≥ 15 kV/mm | ≥ 30 kV/mm |
| Chemical Resistance | Good | Good | Excellent (sealed) | Excellent |
| Moisture Protection | None | None | Sealed (adhesive barrier) | Excellent |
| Sterilization Compatible | EtO, Gamma (limited) | EtO, Gamma (limited) | Limited | All methods including autoclave |
| Typical Medical Use | General wiring, equipment harnesses | Patient-area installations, enclosed racks | Outdoor/underground medical facility feeds | Surgical instruments, sensors, sterilization equipment |
| Relative Cost | $ | $$ | $$ |
The selection decision hinges on where the tubing sits in the facility hierarchy. A dual-wall adhesive-lined tube makes sense for the buried cable feeds entering the hospital building, where moisture ingress is the dominant concern and smoke generation in a fire is less critical because the cable is underground. The same tube would be a poor choice inside an MRI suite or operating room equipment rack, where an LSZH single-wall tube — producing minimal smoke and zero acid gas — is the only defensible option. Fluoropolymers offer unmatched temperature and chemical resistance but come at a premium; they are reserved for applications where those properties are non-negotiable, such as sensor cabling inside autoclaves or surgical tool wiring exposed to repeated sterilization cycles.
Key Applications Across the Hospital
Flame-retardant heat-shrink tubing appears in virtually every electrical subsystem within a modern hospital. The specific requirements vary by location.
Patient Monitoring and Diagnostic Equipment. Bedside monitors, ECG machines, pulse oximeters, and infusion pumps contain densely packed internal wiring harnesses. IEC 60601-1 mandates that internal wiring insulation meet FV-1 flammability classification or better. Flame-retardant heat-shrink tubing — typically single-wall LSZH polyolefin at 2:1 shrink ratio — is used to insulate solder joints, crimped terminals, and wire-to-connector transitions throughout these devices.
Imaging Systems. MRI, CT, and X-ray equipment present extreme environments: high voltages, strong magnetic fields, and stringent electromagnetic compatibility requirements. Heat-shrink tubing in these systems must combine flame retardancy with high dielectric strength. Fluoropolymer tubing is common where cables enter the gantry or patient bore, where temperatures can spike and chemical cleaning agents are used daily.
Operating Room Equipment. Surgical tables, anesthesia machines, endoscopic towers, and robotic surgery platforms all contain cable harnesses that must withstand repeated cleaning with aggressive disinfectants while maintaining flame-retardant performance. LSZH tubing is the standard choice here, as any halogenated material that could off-gas corrosive compounds during cleaning or in a fire event is unacceptable in an OR environment.
Building Infrastructure and Essential Electrical Systems. NFPA 99 requires hospitals to maintain essential electrical systems (EES) — life safety, critical, and equipment branches — with backup power and fault tolerance. The cable terminations and splices in these systems, from generator connections to transfer switches and distribution panels, are protected by flame-retardant heat-shrink tubing, often dual-wall adhesive-lined for outdoor or below-grade installations. A failure in these connections during a fire could disable the very systems patients depend on.
Nurse Call and Communication Systems. While lower voltage, these systems run through every patient room and corridor in the facility. A fire originating in a nurse call cable junction can spread through the entire low-voltage wiring infrastructure. Flame-retardant tubing at every splice point contains the risk.
Selection Criteria for Procurement and Engineering Teams
Choosing the right flame-retardant heat-shrink tubing for a medical application requires evaluating five factors in sequence. The order matters, because each decision constrains the next.
1. Regulatory Pathway. Is the tubing going into a certified medical device (IEC 60601-1 scope) or into a facility’s building wiring (NFPA 70 / NFPA 99 scope)? The former demands biocompatibility documentation and FV-1 or better flammability; the latter prioritizes LSZH composition and VW-1 rating.
2. Fire-Load Environment. How much combustible material surrounds the installation point? A cable tray packed with 50 cables above a suspended ceiling in a patient ward is a much higher fire-load scenario than a single wire in a spacious equipment cabinet. The higher the fire load, the more critical LSZH becomes.
3. Environmental Stressors. Temperature cycling, chemical exposure (disinfectants, sterilants, bodily fluids), mechanical abrasion, and moisture all dictate material choice. A silicone-based flame-retardant tube may handle heat better than polyolefin but typically falls short on mechanical durability; a polyolefin LSZH tube balances most factors for interior use.
4. Shrink Ratio and Dimensional Fit. A 2:1 shrink ratio covers most wire-to-wire splices. But transitions from a thin wire to a bulky connector body may require 3:1 or 4:1 tubing to achieve a tight seal at both ends. Mismatched shrink ratios lead to loose fits that defeat both electrical insulation and flame barriers.
5. Supplier Documentation. A UL file number printed on the tube is not enough. For medical applications, request the full test report: UL 224 VW-1 data, UL 94 classification for the specific wall thickness, halogen content analysis per IEC 61249, and — where applicable — ISO 10993 biocompatibility test results. A manufacturer that cannot produce these documents on request should not supply components for a healthcare facility.
Willele: Engineered for the Demands of Medical Environments
At Willele, we manufacture flame-retardant heat-shrink tubing with the documentation discipline and batch-level traceability that medical equipment manufacturers and hospital engineering teams require. Our FR-series polyolefin tubing carries full VW-1 certification under UL 224 and is available in LSZH formulations that comply with IEC 61249 halogen-free thresholds. Every production batch is tested for flame retardancy, dielectric strength, and dimensional consistency before shipment.
For medical device OEMs, we provide cut-to-length tubing, custom printing, and kitting services that integrate directly into your assembly workflow. For hospital facility engineering, we supply bulk spools and pre-cut pieces with full certification packages for your compliance records.
We understand that in a hospital, a few millimeters of polymer around a wire is never just a piece of tubing. It is a fire barrier, an electrical insulator, and a contributor to the facility’s overall life safety strategy. Our products are built to that standard.
Frequently Asked Questions
What is the difference between flame-retardant and flame-resistant heat-shrink tubing?
Flame-retardant materials are designed to slow ignition and self-extinguish once the external flame source is removed. Flame-resistant materials are formulated to resist ignition entirely and are typically used for textiles and personal protective equipment rather than electrical insulation. For heat-shrink tubing in medical applications, flame-retardant is the correct specification; look for UL VW-1 or UL 94 V-0 ratings.
Does all medical-grade heat-shrink tubing need to be halogen-free?
Not necessarily, but in practice it is strongly recommended. Any tubing installed in occupied patient areas, enclosed equipment racks, or operating rooms should be LSZH to avoid toxic gas release and smoke obscuration during a fire. The only common exception is fluoropolymer tubing used in specialized surgical or sterilization equipment, where chemical resistance requirements override halogen-free preferences — and even then, the application must be justified through a risk assessment.
What shrink ratio is adequate for medical device wiring?
A 2:1 ratio covers most internal wiring splices and terminations. For cable-to-connector transitions where the diameter step is large, a 3:1 or 4:1 dual-wall tube provides a tighter seal. The key is to select a tube whose recovered (shrunk) diameter is smaller than the smallest substrate diameter in the assembly.
Is single-wall or dual-wall tubing better for hospital applications?
Single-wall tubing is preferred for most interior medical applications because it is thinner, more flexible, and — in LSZH formulations — carries the full flame-retardant and low-smoke benefits without additional materials. Dual-wall (adhesive-lined) tubing is reserved for outdoor cable feeds, underground conduits, and locations where moisture sealing is the primary requirement.
What certifications should I ask for when sourcing flame-retardant heat-shrink tubing for a medical facility?
At minimum: UL 224 / VW-1 flame test report, UL 94 classification for the specific wall thickness, and a halogen content analysis per IEC 61249 for LSZH claims. For medical device applications, also request ISO 10993 biocompatibility data and IEC 60601-1 flammability compliance documentation (FV-1 or better). A reputable manufacturer will provide these proactively, not just when asked.
